Published in November 1989
GUIDED
PERIODONTAL REGENERATION WITH AN AMNIOTIC MEMBRANE AND FIBRIN GLUE
GUSTAVO
PETTI
Physician and Surgeon specializing in Dentistry. Periodontist.
Piazza Repubblica 4, 09129 Cagliari, Italy.
tel ++39 070 498159, fax ++39 070 400164
web site www.gustavopetti.it
Physician and Surgeon specializing in Dentistry. Periodontist.
Piazza Repubblica 4, 09129 Cagliari, Italy.
tel ++39 070 498159, fax ++39 070 400164
web site www.gustavopetti.it
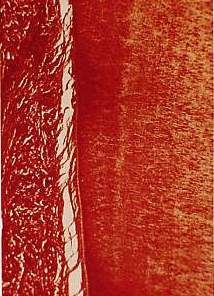
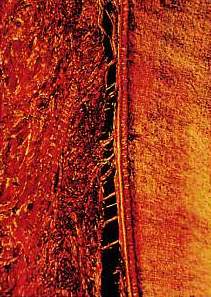
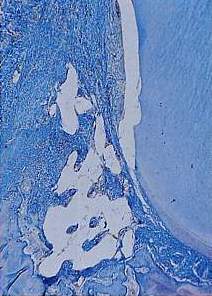

Fig. 32 The stronger enlargement shows the step where the apical cement stops and the lack of amorphous material between the cement and the periodontal connective tissue. Signs of the presence of the bone inducer show up as white (picro-sirius-hematoxylin).


It is beyond doubt that with this technique it is possible to create the conditions for the formation of a short epithelial attachment, the formation of new cement, a new periodontal ligament and new bone formation around and inside the canaliculi of Interpore 200, thus obtaining the new attachment.
References
- BOWERS, G.M.: "Histological evaluation on new attachment in humans", Communication in Periodontal Symposium 30th Anniversary oS Pennsylvania University, giugno 1985
- GOTTLOW, J.; NYMAN, S.; LINDHE, J.; KARRING, T.; WENNSTROM, J.: "New attachment formation in the human periodontium by guided tissue regeneration. Case reports", J. of CL Period., 6: 604-615, 1986
- Karring, T.; NYMAN, S.; LINDHE, J.: "Healing following implantation of periodontitis affected roots into bone tissue", J, of CL Period., 7: 96, 105, 1980
- ISIDOR, F.; KARRING, T.; NYMAN, S.; LINDHE, J.: "The significance of coronal growth of periodontal legament tissue for new attachment formation", J. of Cl. Period"2: 145-150, 1986
- ELLEGAARD, B.: "Bone grafts in Periodontal Attachment procedures", J. of CL Period., 5 (extra issue), 1976
- KENNEY, E.B.; LEKOVIC, V.; HAN, T.; CARRANZA, J.R.; DIMITRISEVIC, B.: "The use of a Porous Hydroxylapatite Implant in Periodontal Defects. Clinical results after six months", J, of CL Period., 2: 56-82, 1985
- LINDHE, J.; WESTFELT, E.; NYMAN, S,; SOCRANSKJ, S,; HEIJL, L.; BRATTHAL, G,: "Healing following surgical/non surgical treatment of periodontal disease", J. of CL Period., 9, 1982
- MAGNUSSON, J.; NYMAN, S.; KARRING, T.; ELGEBERG, J.: "Connective tissue attachment formation following exclusion of gingival connective tissue and epithelium during healing", J. of Periodontal Research, 20: 201-208, 1985
- NYMAN, S.; "New attachment position based on the principle of guided tissue regeneration", Communication in 3rd SIdP International Congress, Milano, 4-7 giugno 1986
- NYMAN, S.; KARRING, T.,' LINDHE, J.,' PLANTEN, S.; "Healing following implantation of periodontitis affected roots into gingival .connective tissue", J. of Cl. Period., 7: 394-400, 1980
- NYMAN, S.: "Guided tissue regeneration in new attachment procedures", Communication in Periodontal Symposium 30th Anniversary of Pennsylvania University, giugno 1985
- PETTI, G,: "Le metodiche attuali pei il trattamento chirurgico ricostruttivo dei difetti ossei", Il Dentista Moderno, 5: 817-832, 1986
- PETTI, G.: "L'impiego della membrana amniotica a protezione della zona donatrice di un innesto libero", II Dentista Moderno, 5, 895-897, 1986
- PETTI, G.: "L'impiego della membrana amniotica in chirurgia ossea", Il Dentista Moderno, 9: 45-50, 1986
- PETTI, G.: "L'impianto di idrossiapatite microporosa con conservazione della papilla a protezione della zona ricevente", Il Dentista Moderno, 4: 667-677, 1986
- PETTI, G.: "Considerazioni sull'uso della membrana amniotica", Il Dentista Mocterno, 1: 97-102, 1987
- PETTI, G., "New attachment. La rigenerazione parodontale guidata con l'uso della membrana amniotica e della colla di fibrina: evoluzione di un pensiero", Piccolo Atlante di Parodontologia, cap. VIII: 57-62, Edizioni Ellebi s.r.l., 1987
- PETTI, G.: "Una nuova tecnica per isolare lo spazio parodontale in chirurgia ossea",Il Dentista Moderno, 3: 425-434, 1988
- PETTI, G.: "L'impiego della colla di fibrina in odontostomatologia", Il Dentista Moderno, 9: 1889-1908, 1987